Native American Foods: Eating and Gathering Habits Explored

Native Americans cover a vast people. Tribes would eat different food depending on their region. Alaskan tribes certainly had a different diet than tribes in the Amazon rainforest. Semi-nomadic tribes would enjoy a changing diet while others would rely on agriculture as their main source of food.
But, we do know a lot of the basics of Native American foods.
Gathering of Food
Supermarkets didn’t exist. Natives had to live a life of foraging and hunting if they hoped to survive. Eventually, domesticated animals were raised and killed, but this wasn’t as common of a practice as hunting, farming and gathering.
Hunting and fishing was a part of life.
Every tribe hunted and fished, and this was primarily a male role. The game that was hunted changed depending on the tribe with Native Americans often choosing to stalk:
- Deer
- Rabbit
- Squirrels
Anything was fair “game.” Other tribes were more ambitious, and they would follow larger animals, such as bison or caribou around. These tribes would send out numerous hunters that would work together to scare the animal in an ambush.
Sometimes, the animal would be led off of a cliff before the hunters finished them off and killed them.
 Traps were often laid to trap game, too.
Traps were often laid to trap game, too.
Fishing tribes used canoes, nets, traps and spear to kill marine life. Bows and arrows were also used as a mean of fishing along with harpoons and blow guns.
Gathering was often the job of the women, and this was an evolving practice. Farming allowed the women to have a much easier job than going out to gather food. The women would gather a lot of different items, including:
- Berries
- Fruits
- Roots
- Vegetables
Corn was a farming staple along with squash and beans which made up a large portion of the Cherokee diet. Corn recipes are very common among Native Americans, along with rice and eventually the inclusion of sugars.
Gathering didn’t just include blueberries, which was commonly gathered, too. Tools would also be used to gather maple syrup. Acorns were gathered to make flour.
Meat was fire-roasted and was the main component of Native American diets.
Collecting Water
Water is a vital life source for every culture and people. Collecting water was essential for life, as it is today, but tribes would build their lives around streams and rivers. The natives would be strategic when choosing where to live.
While the water sources may not be used in the same way today, they could provide the natives with water so clean that it could compare even to the most advanced household water systems today, like a water softener shower head packed with all the latest technology. You can find water of a similar quality in the natural environment and the tribes were good at finding it.
Tribes also knew where to find water and would remain cautious not to move too far from the nearest water source.
Water storage techniques were also incorporated into society. Clay pots would often be filled with water and stored to allow for easy access to water. Natives almost always chose to be at least within one day of a water supply.
Stone and mud walls would eventually be used extensively to direct water through valleys and hills. The practice led to soil that was very moist and rich. Rain water harvesting was also in use within some tribes.
And for good reason.
Water was a vital part of a Native American’s diet.
Native Americans, for the most part, would always have water with their meals. Some tribes would have hot chocolate, this was especially true for tribes in Mexico. Chicha, an alcoholic drink that’s made with corn, was drank in Central and South America by some tribes.
Maize, or Indian corn, was the main portion of a Native American’s diet, but there were also other foods eaten, depending on the region, including:
- Tomatoes
- Peppers
- Peanuts
- Potatoes
- Wild rice
- Sunflowers
- Squash
- Chocolate
- Papaya
Food was eaten fresh, and spices weren’t used extensively. Eggs, if available, would be eaten by Natives, too. Mexico and Central American tribes were different in this way. Instead, tribes in these areas used an abundance of spices and would eat meat that often wasn’t as fresh as what other tribes ate.
Corn was made into a variety of foods, including breads, tortillas, corn on the cob and baked in clay ovens.
The arrival of Europeans led to new farm animals, crops and farming habits. Buffalo became less of a part of Native American diets, too as Europeans killed off most of the Buffalo.
The Most Popular Native American Boats and How They Were Used

Boats were a common form of travel for Native Americans, and there were several different types of boats used by Native communities. The style used was largely dependent on the tribe. We’re going to take a closer look at the types of boats used, and their purpose.
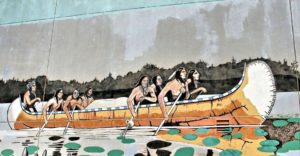
Canoes
Canoes were the most common type of boat used by Native Americans, but this style of boat was also widely used in Central America, South America and the Caribbean.
There were numerous canoe styles used by the Native Americans, and tribes could even recognize one another by the profile of the canoe. But there were three general types used by the Native community:
 Dugout
Dugout
The simplest canoe type is the dugout. Like its name suggests, this boat is made out of hollowed-out wooden logs. Oftentimes, these boats were incredibly simple, with logs being only minimally adapted from their log shape.
Some tribes, especially those in the northwest coast, created more advanced dugout canoes, with intricate wood carvings. These tribes also used special bending techniques that created unique shapes to make the boats quicker.

Plank
Plank boats were far less common, and typically only found in the west. These boats were made of cedar wood planks that were “stitched” together. While these boats had a more complex construction, they were very similar to dugout canoes that were more popular with their neighboring tribes.
Bark
Bark canoes were common in the Northeast woodlands are and the Great Lakes. These lightweight boats were made of either elm or birch bark and stretched over a wooden frame.
Canoes are still used today, and inspired many modern self-propelled boats. Paddles or sticks were used to propel these boats through the water. If you’ve ever been canoeing, kayaking or even a home water rower, you have a good understanding of how Native Americans would navigate the waters.
Sailboats
Although rarely used, sailboats were used by some Native Americans, mainly by tribes in southern Florida. The Ais and Calusa used these boats.
Native sailboats were far more common in South America and Mexico.
Sails were often made from plant fibers and reds, and required very little rigging. They weren’t used for tacking, but rather just for wind sailing.
Bull Boats
Sometimes referred to as coracles or round boats, bull boats were often used by tribes in the plains to transport goods down rivers.
Interestingly, these boats had a bowl-shaped frame made of wood. And as you might have guessed, the exterior of the boat was covered in buffalo skin. The furry side faced outward. Some tribes attached the bison’s tail to the hide, and used the tail as a strap to drag the boat up to the shore.

Because of their round shape, bull boats were difficult to steer and were incredibly slow-moving. But they were easy to build and could carry a lot of weight. Some were able to hold up to half a ton of weight. Its sturdy design made it ideal for the purpose of transporting goods.
Surprisingly, these boats were incredibly light. In fact, they could be carried on your back with ease.
More often than not, Native women built these boats and were the ones responsible for paddling them. Many Native Americans would bring these boats on hunting trips, and ferry their catch home.
Authentic Native American boats are rarely used today, although modern canoes are still popular. Most boats built using Native ways are designed for ceremonial use only.
Thanks to HomeGymSumo for this post, check out their latest rowing machine reviews.
Native American Traditions and Culture Still Going Strong

Throughout the United States, there are 566 Native American and Alaska Native tribes that are recognized by the federal government. Each tribe has its own unique culture, its own cuisine, its own housing style and its own dress. While tribes that are recognized by the federal government vary in population size and location, each is considered a sovereign nation. Each of these nations has its own distinct relationship with the United States.
Plagued by disease and war, much of the Native American population was wiped out by European explorers. But today, Native culture is experiencing a renaissance, with tribes celebrating their traditions and ways.
A War On Culture
Before Europeans arrived in the Americas, Native American tribes were self-governing, and they had been living this way for hundreds of years. Each tribe developed its own methods for teaching their youth and governing their own communities.
Their methods of self-governance were so effective that the U.S. government’s roots can be found in the principles shared by the Iroquois Confederacy.
Unfortunately, Europeans shattered many tribes in their conquest to take over land and resources. Native Americans were forced to relocate from their homelands as a result. Warfare, disease and broken treaties ripped Native communities apart. Many were completely wiped out.
The horrific “Indian Wars” of the 18th and 19th centuries and attacks on Native culture from the U.S. government caused many tribes to lose their lands. Most Native Americans were forced to relocate from the land of their ancestors, where they had been living for hundreds of years, to reservations.
Reservation lands are just a fraction of the size of the lands and natural resources that were stolen from the Native community.
Tribes were split, many forced to integrate with enemy tribes, and moved to reservations that were far from their sacred lands and homes.
Until 1978, Native Americans were prohibited from practicing their ceremonies and religion. The American Indian Religious Freedom Act once again allowed the Native community to practice their traditions, ceremonies and rituals. In 1994, the law was amended to allow the use of peyote during ceremonies. Until 1990, many tribes lost complete control of their human remains and ceremonial items.
 The Boarding School Era, which lasted from the 1800s through the middle 1900s, forced Native children from their homes. The U.S. government forced children from Native communities into Christian boarding schools, oftentimes hundreds of miles from their families. Children faced harsh punishment for speaking their language or practicing their traditions. It wasn’t uncommon for kids to die from disease or malnourishment. Those who managed to survive were completely disconnected for their ways and their families.
The Boarding School Era, which lasted from the 1800s through the middle 1900s, forced Native children from their homes. The U.S. government forced children from Native communities into Christian boarding schools, oftentimes hundreds of miles from their families. Children faced harsh punishment for speaking their language or practicing their traditions. It wasn’t uncommon for kids to die from disease or malnourishment. Those who managed to survive were completely disconnected for their ways and their families.
Many descendants of Natives lost their language and traditions as a result of the Boarding School Era.
Today, many tribes are reviving their cultures and their way of living. Language and ceremony are at the heart of the renaissance. Many tribes are creating programs to teach their languages and dialects. Radio stations are broadcasting in Native languages, powwows are being held across the country, and ceremonies are returning.
Native American Indian Culture: Rituals, Dances and Ceremonies

When European colonists first arrived in “The New World,” there were nearly 12 million Native Americans living in what is now the United States. Divided into more than a thousand different tribes, Native Americans have a rich, diversified culture that is still very much alive today.
Native American Tribes Across the U.S.
Tribes and their cultures varied depending on the region of the country.
Northeast
The northeast consisted of two primary groups: Iroquoian speakers (Oneida, Cayuga, Onondaga, Erie, Tuscarora and Seneca), and Algonquian speakers (Fox, Pequot, Wampanoag, Shawnee, Menominee and Delaware).
Groups in this region lived in small fishing and farming villages along the coast. They grew crops like vegetables, corn and beans.
Southeast
The southeast consisted of several well-known indigenous tribes, including the Chickasaw, Cherokee, Creek, Choctaw and Seminole. These groups were known as the Five Civilized Tribes, and they each spoke a variation of the Muskogean language.

Plains
The plains region stretched from the Rocky Mountains to the Mississippi River, and consisted of the Algonquian, Siouan, Uto-Aztecan, Caddoan and Athabaskan speakers. After Europeans settled in the region, groups like the Blackfeet, Crow, Comanche, Cheyenne and Arapaho became nomadic.
Southwest
The southwest region included New Mexico, Arizona, Utah, Texas, Colorado and parts of Mexico. The peoples in this region had two very distinct ways of life.
The Zuni, Hopi, Yuma and Yaqui were sedentary farmers that grew crops and lived in permanent settlements with kivas, or ceremonial pit houses, at the center of the village.
The Apache, Navajo and other similar tribes were more nomadic. They hunted, gathered and raided established neighbors for their crops.
California and the Northwest Coast
It’s believed that present-day California had more people before European contact than any other area, with an estimated population of 300,000 in the 16th century. There were believed to be over 100 tribes and groups that spoke over 200 dialects in the region.
Despite the complex linguistic landscape, most of the peoples living in this region lived similar lives, with family-based groups of hunters-gatherers.
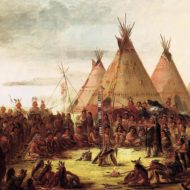
Native American Dances, Rituals and Ceremonies
Dancing is an integral part of the Native American culture and their rituals and ceremonies.

Dances and religious ceremonies are often centered on The Great Spirit, believed by many Native Americans to be the creator of life, or the supreme being. Other Native American traditions, beliefs and religions were based on the culture of shamanism, under which the Shaman or Medicine Man of the tribe served as a medium between the spirit world and the visible world. It is believed that Shamans and Medicine Men had the power to heal the sick, see the future and control the hunt.
Rituals, dances and ceremonies were performed to appease The Great Spirit or the spirits of their ancestors.
Festivals and ceremonies include chanting, singing and dancing. The clothing worn by both the males and females of the tribes were extraordinarily detailed. Some were adorned with furs and feathers, others with color beads and metallic baubles.
Some of the most famous Native American dances include: Deer Dance, Pipe Dance, Rain Dance, Dog Dance, Scalp Dance, Hopi Snake Dance, Green Corn Dance, Sun Dance, War Dance, Ghost Dance, Hoop Dance, Doll Dance and Buffalo Dance.
Indians, or Native Americans? Both Terms are Misleading
When European explorers first landed on the shores of North America, they mistakenly believed that they had landed in India, hence they began incorrectly calling the indigenous peoples Indians.
Unfortunately, the name stuck, and many people still refer to Native Americans as Indians to this day. While there are a select few Native Americans that refer to themselves as Indians, most prefer to use their tribal names.
While Native American is still the preferred term, it’s just as misleading as the term Indian. Both insinuate a homogeneous population when in fact, there were thousands of tribes at the time European explorers came to the Americas. Many of those tribes did not share a common language and had their own cultures. Some tribes were constantly at war with one another. It is likely for this reason that many indigenous peoples of the Americas prefer to use their tribal names, such as Sioux or Lakota or Apache.

As a general rule of thumb, it’s best to ask whether it’s okay to refer to a Native American as Indian so as to avoid offending the person.
A Diverse Range of Tribes
When Europeans first came to the Americas, Native American tribes were found in all corners of the country.
- The Seneca, Delawares, Iroquois, Mohawk, Cayuga, Algonquin and other tribes inhabited the northeast.
- The Cherokees, Seminoles and Miccusuki inhabited the south.
- The Paiute, Shoshone, Mewuk and other tribes were living in California.
- The Sioux, Apache, Comanches and others were living in the southwest.
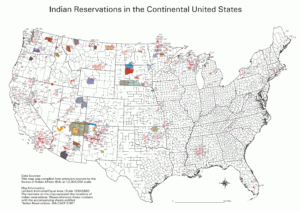
Eventually, the Europeans moved westward, pushing the native peoples out of their homeland. Advanced technology and superior numbers prevailed, and the remaining natives were moved onto what is known as Indian reservations.
There are hundreds of reservations across the United States, and unfortunately, many of the natives that live there today are living in poverty. Some tribes have profited off of the natural resources on their lands and are wealthy. Other reservations run thriving tourist businesses.
While many Native Americans still live on reservations today, not all do. There are a great many that have chosen to integrate into America’s dominant culture.

Visiting Reservations
Visiting a reservation is a great way to learn more about the Native American culture. Not all reservations are open to the public, but those that are typically offer a wealth of information. From museums to hotels, cultural exhibits and more, there’s a lot to experience and explore. Some tribes also allow the public to join in on their ceremonies and dances.
Please note that not all reservations are open to the public and many still wish to preserve their culture and privacy of their homes. There are tribes that also prohibit outsiders from joining in on their dances and ceremonies, so please respect their privacy and wishes.
If you cannot visit a reservation, you may be able to attend a powwow. Most powwows are open to the public, and often include ceremonial dancing, drumming, singing and tribes adorned in their native dress.
When attending a powwow or visiting a reservation, remember to be respectful of name preferences. Some may prefer to be called Native Americans and others by their tribal name. If you are unsure, Native American is the most appropriate term to use.
A Day in The Life of Native Indian Americans

Native American life was a lot different than working a 9 – 5 job, running to the nearest restaurant and ending the day watching television on the couch. Life as a Native American changed for men, women and children.
To get a clear picture of the daily life of Native Americans, we need to look at it from three perspectives:
A Day in The Life of Native Men
The men began their lives with the name of an elder or ancestor. Later in life, their name would change that described a heroic act in their lives. Boys were focused on fighting and horsemanship, so they had little time for girls.
Being tough and brave was essential for men.
Men may join battles, which would consume their lives. The guardian spirit caused men to leave their tribe at the age of 17 in search of the spirit. Upon returning home, he would be ready for battle or would be sent out to hunt for his tribe and family.
Days or weeks would be spent on trying to find herds.
Men would report back to the tribe and then have to go and kill the buffalo if asked. Animals were sacred, and only the number of animals needed to eat were killed.

A Day in The Life of Native Women
Women held a very important role in their society. Women would pitch tipis, move tipis if the tribe was relocating, and they were in charge of tanning hides, too. Skinning buffalo and pray was the job of the women, and they cooked, too.
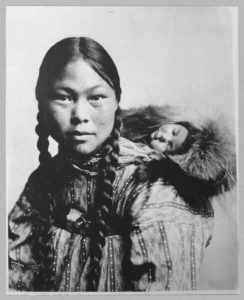
Gathering was the job of women. The women in a tribe would collect berries, nuts and other consumables while the men were hunting.
When the women weren’t working, they would engage in a game of “shinny,” which is a lot like field hockey.
Women were so vital to the tribe that without them, the tribe would cease to exist.
A Day in The Life of Native Children
Children had different roles, depending on the tribe they were part of at birth. Children that were part of the Plains Native tribes were cared for by their parents, and they were never beaten. Strength was vital to the tribe, and crying was not acceptable.

Babies may even have been moved to another location if they cried and wouldn’t stop.
The issue with this practice is that opposing tribes may hear the cries and locate the baby and their respective tribe. Children would eventually be taught in the ways of their tribe and their beliefs.
Rituals would be taught to children, too.
Children copied their parents often to learn how to live and perform daily activities. Boys would be seen on toy horses. Girls would be seen making tipis and played with dolls made out of the skin of deer.
Boys would go out to find their spirit animals between the age of 14 – 17. Much of a boy’s younger years were spent training for hunts and battle.
Rituals and religion were also a major part of life, with tribes honoring their ancestors often and holding big ceremonies when the entire tribe was able to gather together.
About Us

Yvwiiusdinvnohii was created to celebrate, explore and share Native American culture. Our goal is to educate our readers and hopefully provide them with a greater understanding of the Native way of living.
read more